Opening hours
Monday-Friday 7am-7pm
Hamstring Strain Recovery
Outline
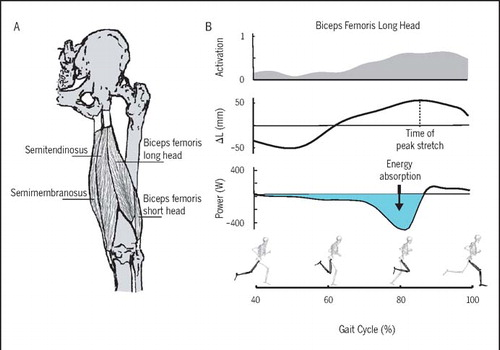
Our Hamstring muscle makes up most of our thigh muscle. At the back of our leg it crosses both our knee and hip joint. Because it crosses two joints, it’s primary action is to flex (bend) the knee and extend (bring leg back) at the hip.
The hamstring is not composed of one muscle but of 3 large muscles:
- Bicep femoris
- Semimembranosus
- Semitendinosus
(https://www.jospt.org/doi/full/10.2519/jospt.2010.3047)
For those of you that run, when you are running at 100% speed, at the terminal swing phase your hamstring muscles are percentage activity is:
-Bicep femoris 67%
-Semi membranisis and semitendinosis at 37%
This is why when we see a running hamstring injury it is usually your bicep femoris.
With hamstring injuries, the most common are hamstring strains (tears) and tendinopathy (tendon overuse injury).
Recovery
Phase 1 – Protection, Ice, and NSAIDs (if prescribed by Dr first few days). Therapeutic exercises consist of neuromuscular and isometrics in a protective range. The physio will give you progression criteria to pass you to phase 2. An example of a progression would be normal walking without pain.
Phase 2 – Protection in this phase – the muscle should be pain free in full range, however, we still avoid passive stretching into full range if weakness is still present. Therapeutic exercises consist of neuromuscular and isometrics in a protective range. Therapeutic exercises include neuromuscular, core stabilization, and strength focusing on eccentric control. All exercises need to be pain free. One example of the progression criteria in this phase would be pain free manual muscle test for the hamstring
Phase 3 – In protection for this phase there is no restriction in passive stretching however, sprinting/accelerating should be avoided until the athlete meets return to sport criteria. Therapeutic exercises should consist of sports specific drills, continuing progression of eccentric strength exercises leading towards end of hamstring range and trunk stability.
Return to sport criteria – In order to return to sport your physio will do some final testing and once you have achieved all the criteria you will be asked to try 2 full training sessions. If there are no impairments such in pain, strength or performance you will be able to return to sport. The hamstring will still be vulnerable 2 months during return to sport. Also, with the recurrence rate of hamstring injury being 2x as likely, it is advised to have a physio monitor your progress throughout your season of sport.
By Physiotherapist, Paulina Backiel







{kind=link}
{kind=link}